










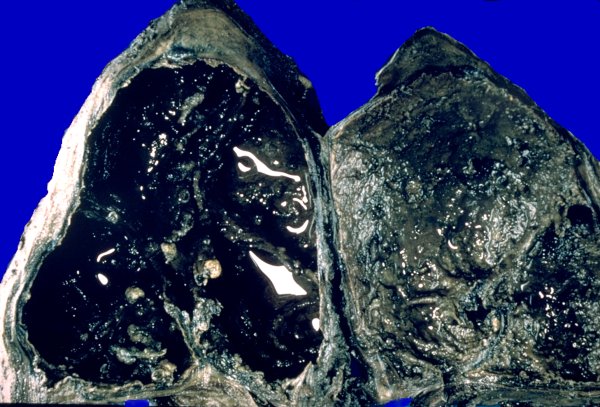

CAVITARY TUBERCULOSIS: Extensive necrosis with cavitation, usually occurring in the upper lung or apex, is a characteristic feature of "secondary" or "adult type" tuberculosis. This is probably related to pre-existing hypersensitivity to M. tuberculosis resulting from a prior primary infection. Cavities form when necrosis involves the wall of an airway and the semi-liquid necrotic material is discharged into the bronchial tree from where it is usually coughed up and may infect others. This infected material may seed other parts of the lung via the airways to produce a tuberculous bronchopneumonia. If swallowed, infection of the G.I. tract may result. Communication of the centers of the tuberculous lesions with the airway exposes the bacteria to a high concentration of oxygen and promotes their proliferation. The risk of spread of infection to non-infected persons from individuals with cavitary tuberculosis is very high.
The following group of photographs illustrate upper lobe/apical cavitary disease:
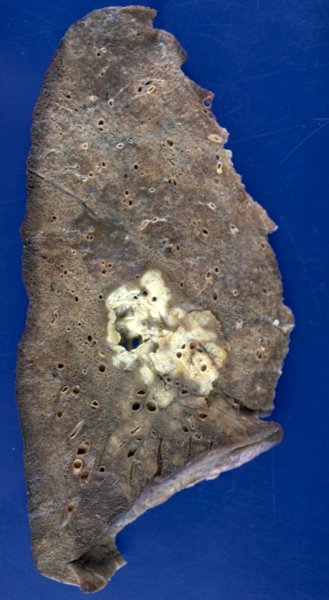
Cavitation and tuberculous bronchopneumonia
Cavitation and tuberculous bronchopneumonia
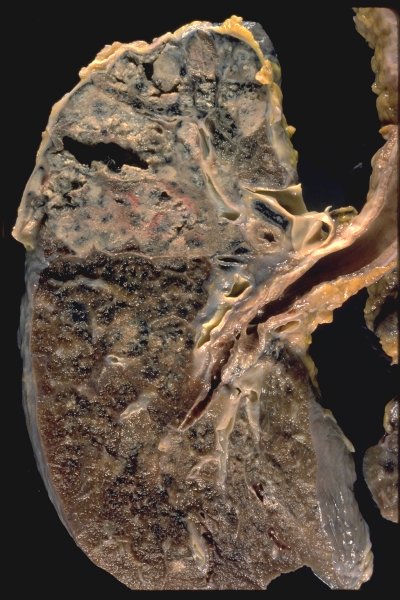
Cavitation
Cavitation and tuberculous bronchopneumonia
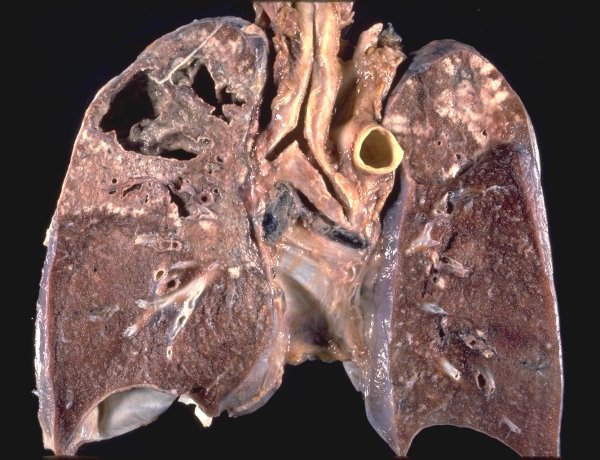
Cavitation and extensive tuberculous bronchopneumonia
Cavitation and extensive tuberculous bronchopneumonia
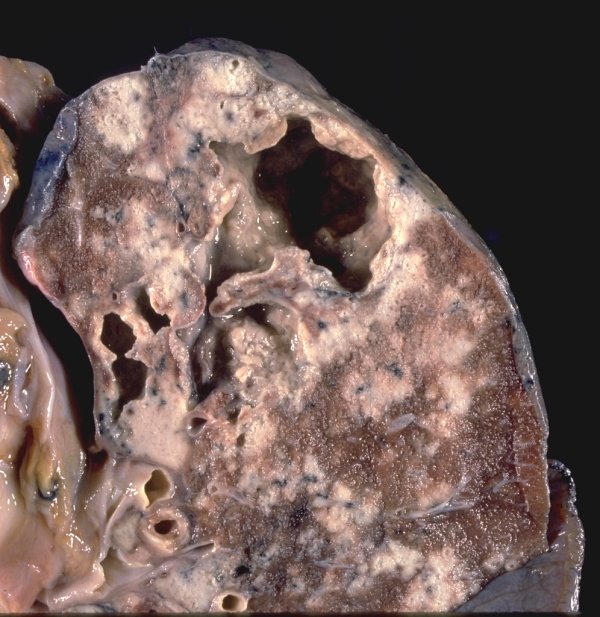
Tuberculous bronchopneumonia associated with cavitary disease
Tuberculous bronchopneumonia associated with cavitary disease
Cavitation in the lower portion of upper lobe
HEMORRHAGE COMPLICATING CAVITARY DISEASE: Erosion of pulmonary or bronchial blood vessels at the periphery of the cavity or traversing it may lead to intracavitary hemorrhage which may, in some cases, be massive and life-threatening
Massive, fatal intracavitary hemorrhage
Extensive intracavitary hemorrhage
HEALING OF CAVITARY LESIONS: With control of the infection and elimination of tubercle bacilli cavitary lesions undergo a healing process which results in their linings undergoing transformation to scar tissue. Old, healed cavities may become colonized by saprophytic Aspergillus sp. forming a "fungus ball" commonly referred to as an aspergilloma.
Apical healed cavity
Apical healed cavity
Huge healed cavity replacing an entire lung
Fungus ball - aspergilloma- occupying and filling an old tuberculous cavity
Small foci of cavitation
Lower lobe cavitation
Click on thumbnail image to view full-size image

Lung parenchyma completely replaced by multiple healed cavities