Granulomas may either involute (resolve) or undergo fibrosis. It has been suggested that emigration of cells, reversion of mature mononuclear phagocytes to less mature forms, and apoptosis play a role in involution. The images on this page illustrate the evolution of fibrosis in sarcoidosis.
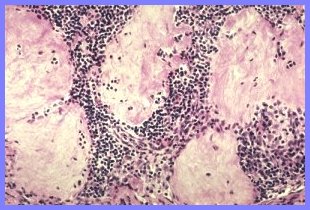
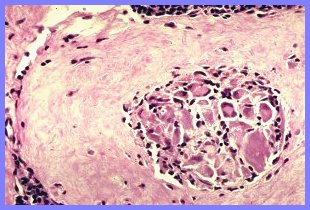
Fibrosis usually begins at the periphery of the granuloma (Fig. 1-right) and progresses towards the center (Figs. 2-4), ultimately resulting in formation of a scar. Where granulomas are discrete and separate from each other the scars conform to the shapes of the pre-existing granulomas (Figs. 1-left, 4). These scars, which are usually recognizable as healed granulomas, are sometimes referred to as "tombstone lesions". When numerous, these "tombstones" appear to form a "graveyard" of granulomas (Fig. 4).
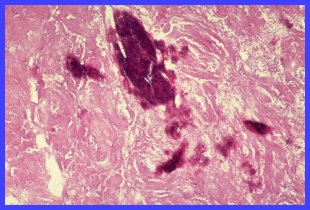
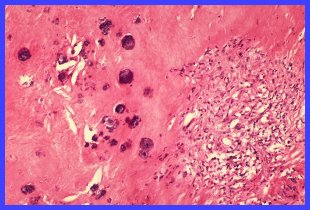
Fibrosis occurring in granulomas which are confluent produces large areas of scarring in which the shape of pre-existing granulomas is not evident (Figs. 6,7). Foci of calcification, either small and discrete (Fig. 6) or plaque-like (Fig. 7) may occur in such scars.
Fate Of Granulomas
Fig. 1. Early peripheral fibrosis at right; complete fibrosis at left ("tombstone lesion")
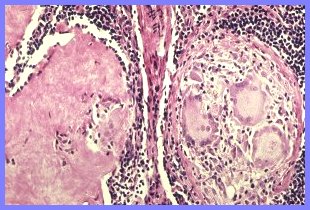
Fig. 2. More advanced peripheral fibrosis at right; sub-total fibrosis at left with only an asteroid-containing giant cell remaining.
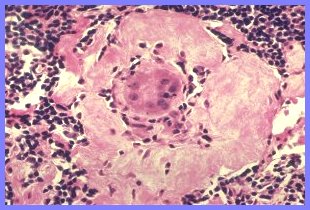
Fig. 3. Peripheral fibrosis advancing towards the center of the granuloma
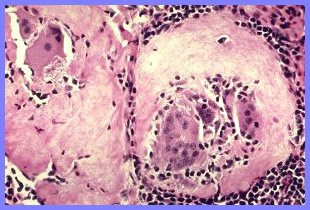
Fig. 4. Subtotal-fibrosis with only a giant cell remaining in the center of the granuloma
Fig. 5 Discrete, totally fibrotic granulomas; a "graveyard' of "tombstone lesions"
Fig. 6 Confluent scarring with small, discrete foci of calcification. Residual granuloma at right.
Fig. 7 Confluent scarring with larger, plaque-like foci of calcification. No evidence of pre-existing granulomas.